Are there procedures or operations
that can help?
It is possible to improve the urethral support that has become weak resulting in stress incontinence. There are three ways that this can be done:
• Placing a tape under the urethra to support the urethra when there is stress incontinence – Tension Free Vaginal Tape or Transobturator tape
More info
• Fixing the bladder in a higher position by stitches placed at an operation (eg Burch colposuspension) - this is the traditional way to treat stress incontinence
More info
• Autologous Pubovaginal Sling – using your own tissue from the abdomen and placing it
under the urethra to support the urethra when there is stress incontinence
More info
• Injecting agents to increase the bulk of the urethral wall
More info
In some cases, these can improve symptoms of urgency or urge incontinence, but you need to have a careful discussion with your doctor.
For people who suffer with a strong urge to pass urine that does not respond to simple drugs and medication, BOTOX injections can significantly relax the bladder easing such symptoms. It is a well tolerated procedure, but needs to be repeated every 4 to 9 months.
What is Botox?
Botox is the brand name for botulinum toxin. Botox is used to relax muscular tissue and is commonly used for wrinkles on the face. In the bladder, it can relax the bladder muscle. This results in a reduction in the need to visit the toilet as frequently as one did before.
Who is suitable for treatment with Botox?
Men or women who have to pass urine too frequently or rush to the toilet to pass urine, especially during the day and night may be suitable for Botox. A test called urodynamics is performed first to determine whether the bladder muscle ('detrusor') contracts inappropriately i.e. when the bladder is meant to be storing urine. If the bladder is proven to be contracting inappropriately, drugs are tried first to calm the bladder muscle. These drugs are known as anticholinergic drugs and include tolterodine (Detrusitol), solifenacin (Vesicare) and oxybutynin (Lyrinel).
If the medications do not work, then it is necessary to know whether the bladder has a reduced physical size. This is determined by filling the bladder up under a short general anaesthetic and seeing how much it can hold. There are no cuts or incisions when this is done. If the bladder is of normal size, then Botox can be performed. If not, it may be better to have an operation to enlarge the size of the bladder.
As Botox weakens the bladder muscle, I usually recommend that people learn how to pass a specially designed catheter themselves before Botox is given. This is because the bladder may temporarily be unable to completely empty and this occurs in about 1 in 10 to 1 in 20 people. may be the easiest way to empty the bladder.
A catheter will not be needed forever, as Botox wears off after 4 to 9 months anyway. The technique is known as intermittent self catheterisation (ISC or CISC) and is tolerated very well by the majority of people who do this. If ISC is not possible for whatever reason, it may not be sensible to perform Botox for the bladder.
Typically, people with an overactive bladder due to detrusor instability or a neurological problem such as multiple sclerosis or a stroke are suitable providing the conditions described above are met.
How is Botox given?
The procedure is a day case procedure, so patients are admitted onto the ward on the day that Botox is administered. No drinking or eating is allowed 5 hours before the procedure. No other special preparation is necessary.
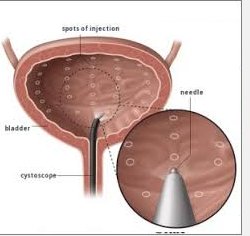
Botox can be given either when asleep ('general anaestheisa') or with the bladder made numb ('local anaesthesia') Under a general anaesthetic, a telescope examination of the bladder is performed ('cystoscopy'). The telescope is passed through natural passage ways in the bladder, so there are no incisions. The bladder is examined carefully. Botox is injected into the bladder wall through a special needle passed through the telescope directly. The bladder is emptied afterwards. Sometimes, a catheter is placed to empty the bladder - this is a small tube to drain the bladder that is removed on the ward.
What should I expect after Botox has been given?
It is possible to eat and drink shortly after the Botox has been given, and you should be able to go home the same day.
You should notice a reduction in the urgency and frequency of going to the toilet to pass urine about 5 days after it has been given. If leakage occurred before Botox, there should be no leakage afterwards. The maximum benefit is obtained about two weeks after the administration of Botox and the total effect lasts for between four and nine months.
What are the side-effects of Botox?
There are few reported side-effects.
Blood may be seen in the urine after injections of Botox, as a needle penetrates the bladder wall. The blood may appear for a few days, but always wears off after a while. An infection may develop in the urine, but antibiotics are given to avoid this.
About 1 in 10 to 1 in 20 people describe a difficult in completely emptying the bladder. In some of these people, it may be necessary to pass a catheter intermittently (ISC). This is well tolerated by most and is not necessary for more than a few weeks in the vast majority.
Allergic reactions are reported, but again these are very rare.
Very rarely, if Botox is injected directly into a blood vessel, breathing might stop. This would not occur immediately, but be noticed slowly over the next few weeks usually within time to act. Appropriate treatment would be administered.
What are the alternatives to Botox?
The alternatives include:
• Cystoscopy and hydrodistension: this means stretching the bladder under general anaesthetic by trying to overfill it with water. This is well tolerated in the majority and rarely causes problems. This can be tried a few times, but does not last very long.
• Bladder augmentation: this means that the bladder is physically made larger. To do this, a segment of intestine is reshaped and fitted onto the bladder to increase its size. This is a fairly big operation, although it can be performed using key-hole techniques.
• Take no action: as this is not a life-threatening problem, treatment is not necessary to prolong life, although it may improve the quality of life. |




