Urodynamics in men with an enlarged prostate |
||
|
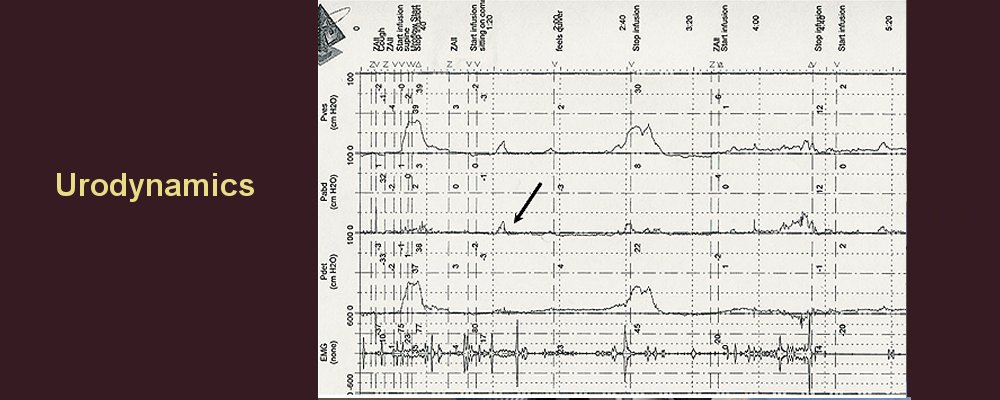
This is a one-hour outpatient diagnostic test to help understand why urinary symptoms are present and to help predict the outcome of treatment. The tests aims to determine the activity of the bladder whilst it is filling with fluid, and the pressure and speed at which urine is passed.
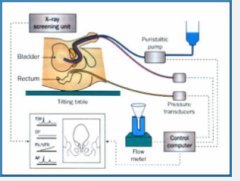
To do this, a very narrow tube has to be passed into the bladder through the urethra. Sometimes, it is combined with x-rays and is known as 'videourodynamics'. A gel with local anaesthesia may be used, but not general anaesthesia. Pressures are measured in the rectum (a.k.a. back passage) at the same time through another narrow tube.
Why am I having this test?
The test can determine the cause of urinary symptoms such as:
It can also help predict whether drugs or surgery are likely to have a good result for:
What should I do before this test?
If you are taking drugs for your prostate or bladder, you should probably stop these a week before having the test. Check first with the nurses or doctors.
These include:
It is not necessary to fast the night before or take laxatives. As long as a urine test to test for infection is normal, the study is very safe and can be performed with minimal discomfort. It is important to arrive with an almost full bladder since it may be necessary to do a urinary flow test before the formal urodynamic test. Usually, a nurse will be in the room during the study. Occasionally, a radiographer or doctor may be there also. What will happen during the test?
For more information, download from the following link:
Are there any medicines that can help symptoms due to an enlarged prostate?
Finasteride or Dutasteride can reduce the size of the prostate by about 20%, and improve symptoms in about 30 percent of patients who take it. Symptom scores improve by about 4 or 5 points out of 25. For example, if your symptom score was 16, then the symptom score would be about 11 or 12 out of 35 after 6 months or more of treatment. The chance of needing surgery for the prostate or being completely unable to pass urine ('acute urinary retention') is reduced by about 50%. To remain effective, the drugs need to be taken for the rest of your life. The side effects of finasteride include reduced volume of semen and altered semen quality, impaired erections, reduced libido, and occasional growth of the breast tissue.
Using finasteride and an alpha-blocker together is more effective than either drug alone to relieve symptoms and prevents BPH getting worse. The two-drug regimen reduced the risk of BPH progression in two out of three patients, compared to one-in three for an alpha-blocker alone and one in three for finasteride alone.
Drugs or medicines may not be enough, and more effective treatments such as a TURP or the HOLEP, may be more suitable. Should I have an operation?
At one time, BPH was invariably thought to be a progressive disease. That is no longer the case. Only about 40 to 50 percent of all men with BPH actually develop any symptoms due to this condition, and of that number, only a proportion will need prostate surgery. BPH requires treatment only if the symptoms are severe enough to disrupt your life or threaten your health.
If, during your prostate examination, your doctor finds that you have significant symptoms and that your prostate gland is enlarged, you may start a program of medication and changes in life style to improve your symptoms. During this time, your doctor may examine you periodically and ask you to complete questionnaires (e.g. IPSS).
If your urination problems are not adequately relieved by medication or the side effects of the drug are excessive, you might then consider a TURP or laser prostatectomy(HOLEP). TURP removes the prostate via a key hole surgery and HOLEP utilises a laser to remove prostate tissue. Removal of the enlarged part of the prostate is the best long-term solution for patients with BPH. Surgery usually relieves the obstruction and incomplete emptying caused by BPH more than any other treatment.
For certain patients with particular signs and symptoms, a TURP or laser prostatectomy is almost always recommended. These signs and symptoms include:
If you decide to have a prostatectomy for reasons of comfort or for a more severe indication, you should know that an operation offers the greatest chance of getting rid of your symptoms. Are there any alternatives to TURP or laser prostatectomy for BPH?
Rezum utilises steam for ablating the tissue. Urolift is another less invasive procedure( which essentially is placing staples in the prostate) and another alternative is prostate artery embolization (PAE) which utilises the principle of placing coil in the blood vessels supplying prostate which shrinks the prostate What are the risks/benefits of surgery?
Although there are nonsurgical treatments available to treat BPH, an operation offers the highest chance of alleviating prostate problems. However, it also can result in problems either during or after surgery.
After a TURP or laser prostatectomy, some men will find that semen does not go out of the penis during orgasm. Instead, it passes into the bladder and is passed with the urine next time. The feeling of orgasm stays the same. This backwards ejaculation is a problem for couples who want to have a baby.
Some conditions after TURP or laser prostatectomy may require additional treatment including: . These risks and benefits must be considered by anyone considering a prostate operation, and your doctor can help you make your decision. How do I decide what treatment is necessary?
The HOLEP laser prostatectomy and TURP are more effective than drugs. In general, HOLEP laser prostatectomy and TURP are most likely to be effective if the prostate is causing obstruction of the bladder. This can be determined by the tests listed above.
Severe and bothersome urinary symptoms
For severe urinary symptoms (IPSS 20 or more) that are bothersome (4 or more out of 6), it is important to look in the bladder to make sure there are no other problems. Further tests to determine whether urinary symptoms are due to obstruction by the prostate will often be necessary, especially if a TURP or other surgical procedure is being considered.
The biggest improvement in symptoms and quality of life occurs with the HOLEP or TURP, but not everyone wants these procedures. Medicines such as alpha blockers or finasteride/dutasteride also relieve symptoms, but not as much. If drugs are used alone, further treatment is necessary. A poor response to alpha blockers and increasing residual urine or symptoms mean that surgery is almost always necessary . In addition, if surgery is delayed when the bladder is obstructed by the prostate, the benefit of surgical procedures may be less than when surgery is performed early. This is possibly because the bladder may undergo irreversible changes if it is blocked for a long period of time. With less invasive treatments available now (eg Rezum, Aquablation, PAE and Urolift), it may be better to opt for one of these earlier than later. How do I decide between drugs or surgery?
Conservative treatments and drugs such as alpha blockers work best when symptoms are mild or moderate. If symptoms are severe and the prostate is causing a blockage, then HOLEP or TURP surgery is more effective and lasts longer than drugs.
The severity of symptoms is judged best by assessing the symptom score (IPSS). If the symptom score is 20 or more and the symptoms are bothersome (4 or more). A test called urodynamics can determine if there is a blockage or not, and can also tell if the bladder contracts at the wrong time.
Sometimes, urinary symptoms such as getting up at night or having to rush urgently to pass urine are not due to the prostate; these symptoms may be due to the bladder contracting inappropriately. Urodynamics can help predict if the HOLEP or TURP may help.
The HOLEP or TURP is most effective when there is obstruction present and this is usually proven by urodynamic testing.
Other factors are also important such as general fitness. It may not be safe to have an anaesthetic, which is necessary for a TURP or HOLEP. Drugs may be the only treatment possible. Occasionally, other procedures are also possible such as 'stents'.
What about Saw Palmetto?
Saw palmetto (Serenoa repens) is a type of palm tree, also known as the dwarf palm. Its primary medicinal value lies in the oily compounds found in its berries. Most dietary supplements are composed of an extract from the berries or a berry powder.
Saw palmetto dietary supplements improve urinary flow, and reduce the frequency and urgency of urination in men with prostate enlargement. Saw palmetto is believed to inhibit the actions of testosterone in the prostate that cause prostate enlargement and interference with urinary flow.
Fatty acids and sterols found in Saw palmetto inhibit testosterone in the prostate. Sterols are also present in other herbs (such as pygeum bark, stinging nettle root, and pumpkin seed extract) used in treating symptoms of prostate enlargement.
Saw palmetto is commonly used in Germany and other parts of Europe and the United States, but less commonly in England. There have been concerns about the quantity of active agent in various preparations of Saw palmetto.
|
|
|
Summary |
|




 What are urodynamics?
What are urodynamics?